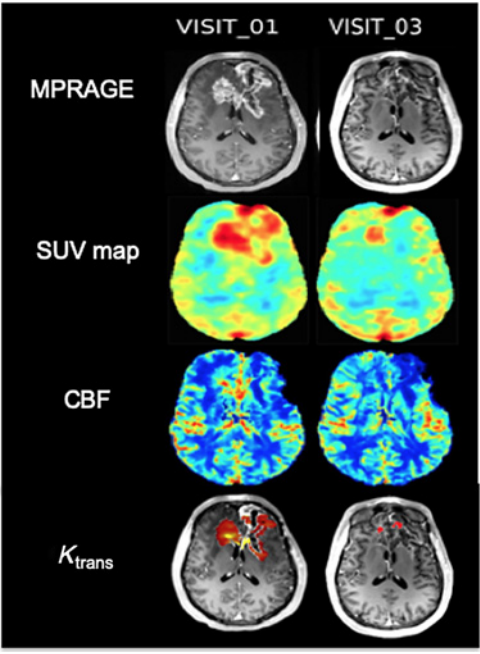
Targeting tumor blood vessels is an attractive therapy in glioblastoma (GBM), but the mechanism of action of these agents and how they modulate delivery of concomitant chemotherapy are not clear in humans. We sought to elucidate how bevacizumab modulates tumor vasculature and the impact those vascular changes have on drug delivery in patients with recurrent GBM. Bevacizumab led to a decrease in permeability and concomitant delivery of temozolomide. However, in subregions of the tumor where permeability was low, increased perfusion improved delivery of temozolomide, suggesting that perfusion may modulate the delivery of chemotherapy in certain settings. These results support exploring whether lower doses of bevacizumab improve perfusion and concomitant drug delivery
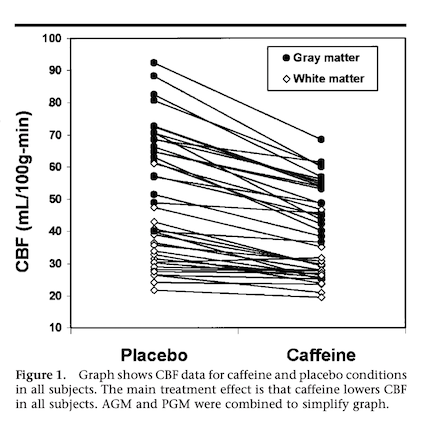
The purpose of this study was to evaluate the effects of dietary caffeine intake and withdrawal on cerebral blood flow (CBF), as determined from a randomized, blinded, placebo-controlled study. Twenty adults (16 men, four women; age range, 24-64 years) categorized as low (mean, 41 mg/d) or high (mean, 648 mg/d) caffeine users underwent quantitative flow-sensitive alternating inversion-recovery perfusion magnetic resonance (MR) imaging twice: 90 minutes after a dose of caffeine (250 mg) on one day and after a dose of placebo on another day (randomized counterbalanced design). Doses were preceded by 30 hours of caffeine abstinence to induce withdrawal in high caffeine users. Quantitative CBF maps were gray matter (GM)–white matter (WM) segmented and subjected to region-of-interest analysis to obtain mean CBF in WM, anterior circulation GM (AGM), and posterior circulation GM (PGM). By using two-way repeated-measures analysis of variance, regional CBF data were tested for within-subject differences between caffeine and placebo and for between-subject differences related to dietary caffeine habits. Linear regression was used to determine whether dietary caffeine use predicts CBF or CBF response to caffeine. It was found that caffeine reduced CBF (P ≤ .05) by 23% (AGM, PGM) and 18% (WM) in all subjects. Postplacebo (withdrawal) CBF in high caffeine users exceeded that in low users (P ≤ .05) by 31% (AGM) and 32% (WM) (PGM, not significant). Mean postcaffeine CBF reduction in AGM was 26% in high users versus 19% in low users (P ≤ .05; PGM and WM, not significant). Increasing caffeine consumption predicted higher CBF (P ≤ .05) in all regions: r = 0.79 (AGM), 0.57 (PGM), and 0.76 (WM). Dietary caffeine use did not predict CBF response to caffeine.
The purpose of this study was to evaluate the effects of dietary caffeine intake and withdrawal on cerebral blood flow (CBF), as determined from a randomized, blinded, placebo-controlled study. Twenty adults (16 men, four women; age range, 24-64 years) categorized as low (mean, 41 mg/d) or high (mean, 648 mg/d) caffeine users underwent quantitative flow-sensitive alternating inversion-recovery perfusion magnetic resonance (MR) imaging twice: 90 minutes after a dose of caffeine (250 mg) on one day and after a dose of placebo on another day (randomized counterbalanced design). Doses were preceded by 30 hours of caffeine abstinence to induce withdrawal in high caffeine users. Quantitative CBF maps were gray matter (GM)–white matter (WM) segmented and subjected to region-of-interest analysis to obtain mean CBF in WM, anterior circulation GM (AGM), and posterior circulation GM (PGM). By using two-way repeated-measures analysis of variance, regional CBF data were tested for within-subject differences between caffeine and placebo and for between-subject differences related to dietary caffeine habits. Linear regression was used to determine whether dietary caffeine use predicts CBF or CBF response to caffeine. It was found that caffeine reduced CBF (P ≤ .05) by 23% (AGM, PGM) and 18% (WM) in all subjects. Postplacebo (withdrawal) CBF in high caffeine users exceeded that in low users (P ≤ .05) by 31% (AGM) and 32% (WM) (PGM, not significant). Mean postcaffeine CBF reduction in AGM was 26% in high users versus 19% in low users (P ≤ .05; PGM and WM, not significant). Increasing caffeine consumption predicted higher CBF (P ≤ .05) in all regions: r = 0.79 (AGM), 0.57 (PGM), and 0.76 (WM). Dietary caffeine use did not predict CBF response to caffeine.
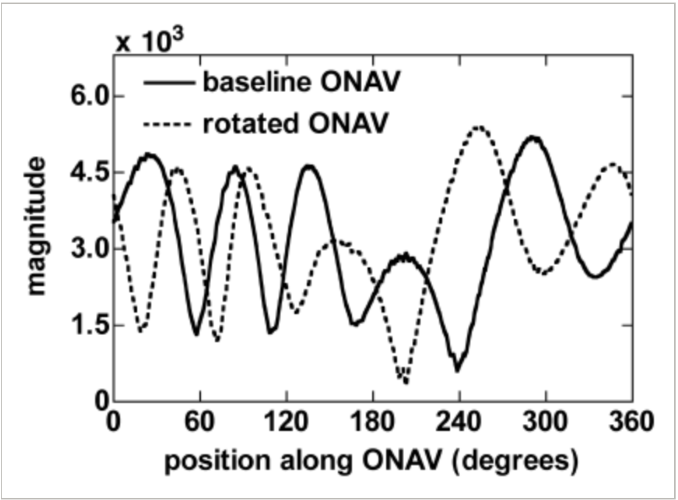
Using the axis of rotation of polar navigator echoes to rapidly measure 3D rigid-body motion
Costa AF et al. Magn Reson Med. 2005;53(1):150-158.
An improved technique to prospectively correct three-dimensional rigid-body motion using polar spherical navigator (pNAV) echoes is presented. The technique is based on acquiring pNAVs of an object in a baseline and rotated position and determining the axis of rotation (AOR) between data sets, thereby reducing 3D rotations to a 2D, planar rotation. Finding the AOR is simplified by prerotating the baseline trajectory, which forces the axis to lie within a specific polar region of a spherical shell in k-space. Orbital navigator echoes are interpolated from the pNAV data in planes orthogonal to the AOR and cross-correlated to determine the 2D rotation. The rotation about the AOR is used in conjunction with its orientation to calculate the overall 3D rotation. The pNAV-AOR technique was tested for its precision, accuracy, and processing speed in detecting compound rotations and translations of varying magnitude. In comparison to the spherical navigator echo technique, the pNAV-AOR technique is noniterative, fast, and independent of rotation magnitude and direction. At low SNR, the technique can detect compound rotations to 0.5 degrees accuracy in an estimated 100 msec, indicating that prospective 3D rigid-body motion correction may be feasible with this technique.
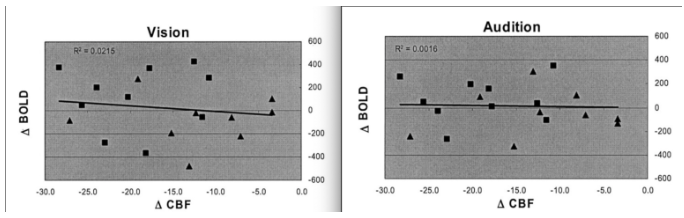
Laurienti PJ et al. Am J Neuroradiol. 2003;24(8):1607-1611.
Recent interest has emerged in the use of pharmacologic methods to maximize blood oxygenation level-dependent (BOLD) signal intensity changes in functional MR imaging (fMRI). Adenosine antagonists, such as caffeine and theophylline, have been identified as potential agents for this purpose. The present study was designed to determine whether caffeine-induced decreases in cerebral perfusion result in enhanced BOLD responses to visual and auditory stimuli. MR imaging was used to measure resting cerebral perfusion and stimulus-induced BOLD signal intensity changes in 19 patients. We evaluated the relationship between resting cerebral perfusion and the magnitude of BOLD signal intensity induced by visual and auditory stimulation under caffeine and placebo conditions. The data showed that changes in resting cerebral perfusion produced by caffeine are not a consistent predictor of BOLD signal intensity magnitude. Although all cerebral perfusion was reduced in all study participants in response to caffeine, only 47% of the participants experienced BOLD signal intensity increase. This finding was independent of the participants’ usual caffeine consumption. Therefore, the data presented shows that the relationship between resting cerebral perfusion and the magnitude of BOLD signal intensity is complex. It is not possible to consistently enhance BOLD signal intensity magnitude by decreasing resting perfusion with caffeine. Future studies aimed at evaluating the relationship between perfusion and BOLD signal intensity changes should seek a means to selectively modulate known components of the neural and vascular responses independently.
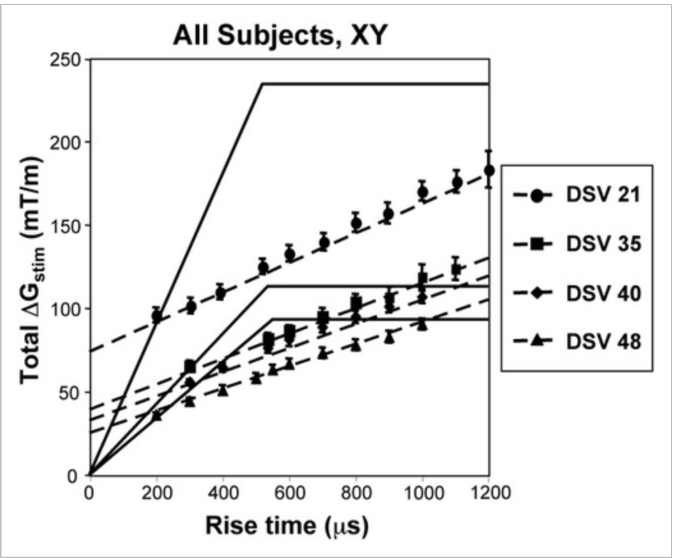
Peripheral nerve stimulation properties of head and body gradient coils of various sizes
Zhang B et al. Magn Respn Med. 2003;50(1):50-58
Peripheral nerve stimulation (PNS) caused by time-varying magnetic fields has been studied both theoretically and experimentally. A human volunteer study performed on three different body-size gradient coils and one head-size gradient coil is presented in this work. The experimental results were used to generate average PNS threshold parameters for the tested gradient systems. It was found that the average stimulation threshold increases while gradient-region-of-uniformity size decreases. In addition, linear relationships between PNS parameters and diameter of homogeneous gradient spherical volume (DSV) were discovered: SR(min) and DeltaG(min) both vary inverse linearly with DSV. More importantly, the chronaxie value was found to vary inversely linearly with the DSV. This finding indicates that, contrary to the general understanding, the parameter “chronaxie” in the commonly accepted simple stimulation models cannot be considered to be a single-value, nerve-specific constant. A modified linear model for gradient-induced PNS based on these results was developed, which may permit, for the first time, the general prediction of nerve stimulation properties for gradient coils of arbitrary linear region dimension.
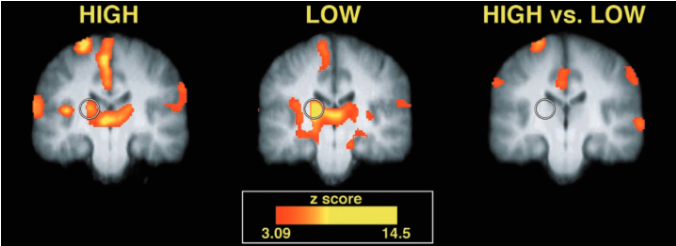
Neural correlates of interindividual differences in the subjective experience of pain Coghill RC et al. Proc Natl Acad Sci USA. 2003;100(14):8538-8542
Some individuals claim that they are very sensitive to pain, whereas others say that they tolerate pain well. Yet, it is difficult to determine whether such subjective reports reflect true interindividual experiential differences. Using psychophysical ratings to define pain sensitivity and functional magnetic resonance imaging to assess brain activity, we found that highly sensitive individuals exhibited more frequent and more robust pain-induced activation of the primary somatosensory cortex, anterior cingulate cortex, and prefrontal cortex than did insensitive individuals. By identifying objective neural correlates of subjective differences, these findings validate the utility of introspection and subjective reporting as a means of communicating a first-person experience.
The purpose of this study was to evaluate the effects of dietary caffeine intake and withdrawal on cerebral blood flow (CBF), as determined from a randomized, blinded, placebo-controlled study. Twenty adults (16 men, four women; age range, 24-64 years) categorized as low (mean, 41 mg/d) or high (mean, 648 mg/d) caffeine users underwent quantitative flow-sensitive alternating inversion-recovery perfusion magnetic resonance (MR) imaging twice: 90 minutes after a dose of caffeine (250 mg) on one day and after a dose of placebo on another day (randomized counterbalanced design). Doses were preceded by 30 hours of caffeine abstinence to induce withdrawal in high caffeine users. Quantitative CBF maps were gray matter (GM)–white matter (WM) segmented and subjected to region-of-interest analysis to obtain mean CBF in WM, anterior circulation GM (AGM), and posterior circulation GM (PGM). By using two-way repeated-measures analysis of variance, regional CBF data were tested for within-subject differences between caffeine and placebo and for between-subject differences related to dietary caffeine habits. Linear regression was used to determine whether dietary caffeine use predicts CBF or CBF response to caffeine. It was found that caffeine reduced CBF (P ≤ .05) by 23% (AGM, PGM) and 18% (WM) in all subjects. Postplacebo (withdrawal) CBF in high caffeine users exceeded that in low users (P ≤ .05) by 31% (AGM) and 32% (WM) (PGM, not significant). Mean postcaffeine CBF reduction in AGM was 26% in high users versus 19% in low users (P ≤ .05; PGM and WM, not significant). Increasing caffeine consumption predicted higher CBF (P ≤ .05) in all regions: r = 0.79 (AGM), 0.57 (PGM), and 0.76 (WM). Dietary caffeine use did not predict CBF response to caffeine.
Diffusion anisotropy in the corpus callosum
Chepuri NB et al. Am J Neuroradiol. 2002;23(5):803-808
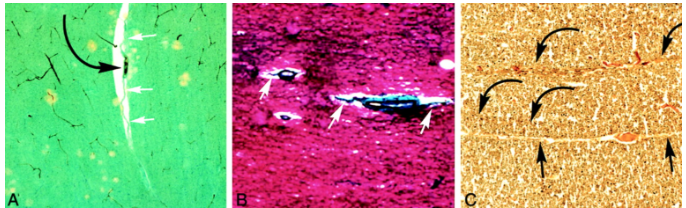
The corpus callosum is a heterogeneous white-matter tract that connects the cerebral hemispheres. The purpose of this investigation was to study its microstructural architecture in normal human adult brains by using diffusion tensor imaging (DTI). Two hundred consecutive patients referred for brain MR imaging underwent additional DTI with a high gradient field strength applied in six directions. Forty-two patients met the following inclusion criteria: 1) normal brain and 2) age greater than 18 years. Anisotropy maps were generated, and regions of interest were drawn around specified regions within the corpus callosum. Results were stratified by sex and age. In addition, available histologic specimens of the corpus callosum from cadaver brains were analyzed with conventional and specialized vascular staining. Results concluded that the anisotropy values in the various regions of the corpus callosum differed significantly. Average values of the anisotropy index for the genus, body, and splenium of the corpus callosum were 0.400, 0.456, and 0.539, respectively. The differences between these values proved to be statistically significant (P <.01), and the results of this investigation show a statistically significant increase in anisotropy of the corpus callosum in its more posterior portions compared with its more anterior portions across sex and age groups. Although the microstructural etiology for this is apparent, increase in anisotropy is unclear due to the number of possible mechanisms presented.
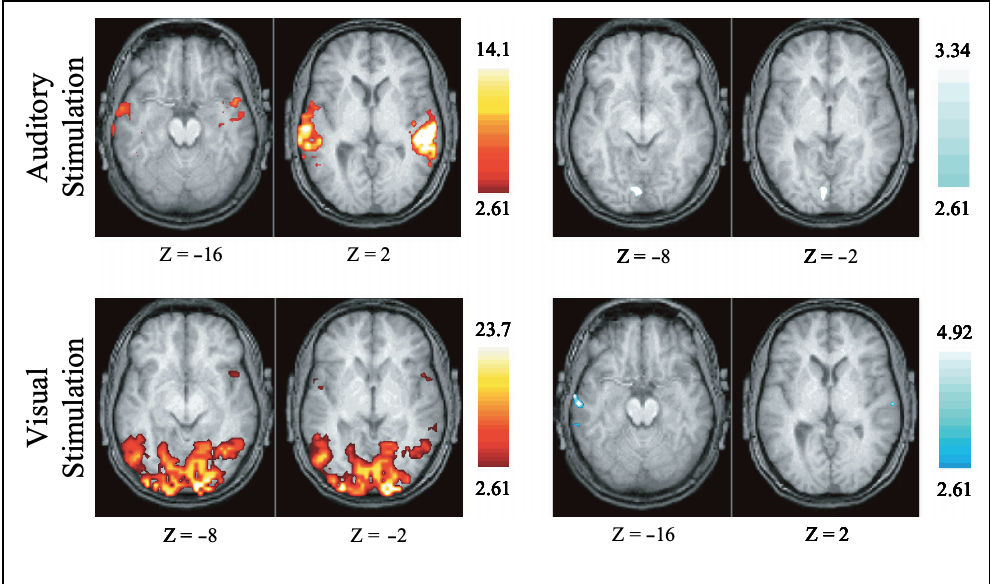
Visual and auditory cortices traditionally have been considered to be “modality-specific.” Thus, their activity has been thought to be unchanged by information in other sensory modalities. However, using functional magnetic resonance imaging (fMRI), the present experiments revealed that ongoing activity in the visual cortex could be modulated by auditory information and ongoing activity in the auditory cortex could be modulated by visual information. In both cases, this cross-modal modulation of activity took the form of deactivation. Yet, the deactivation response was not evident in either cortical area during the paired presentation of visual and auditory stimuli. These data suggest that cross-modal inhibitory processes operate within traditional modality-specific cortices and that these processes can be switched on or off in different circumstances.
Dietary Caffeine Consumption Modulates fMRI Measures
Laurienti et. al NeuroImage October 2002, Pages 751-757
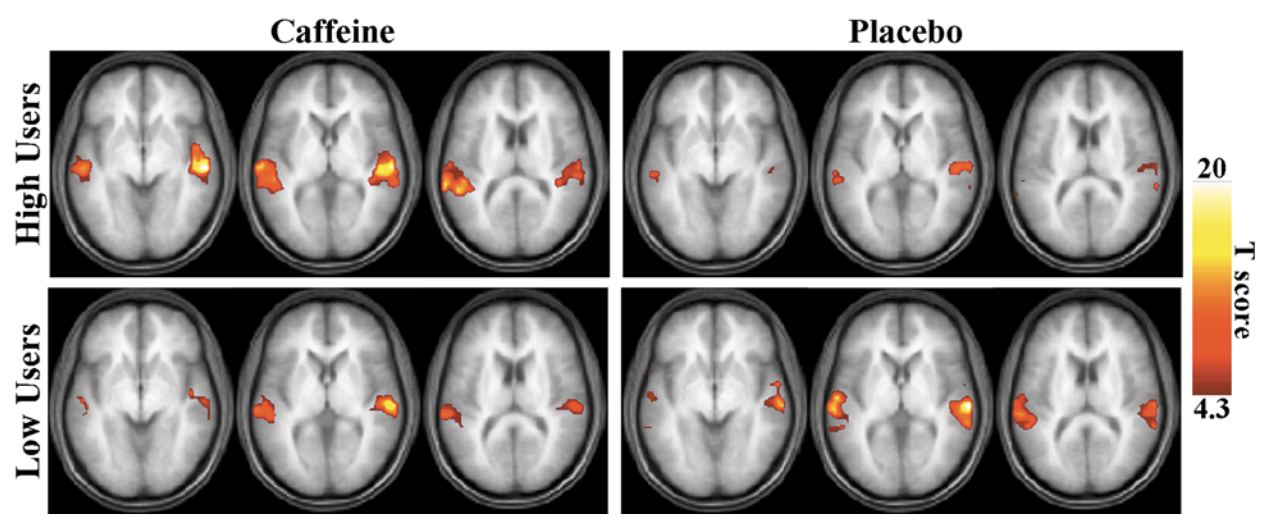
Caffeine is the most widely used stimulant in the world. The stimulant effects of caffeine are mediated through its antagonistic properties on neuronal adenosine receptors. In addition, caffeine blocks neurovascular adenosine receptors and decreases cerebral perfusion. Although the effects of caffeine on blood oxygenation level-dependent (BOLD) functional magnetic resonance imaging measures are extremely important, there are few studies addressing this issue in the literature. Because chronic caffeine use causes an upregulation of adenosine receptors, the differential effects of caffeine in low and high users is of particular interest. The present study was designed to test the hypothesis that caffeine has differential effects on the BOLD signal in high and low caffeine users. We demonstrated that the BOLD signal change in visual cortex was significantly greater in high users than in low users in the presence of caffeine. In addition, the magnitude of the BOLD signal was significantly correlated with caffeine consumption. We propose that the outcome observed here was due to an upregulation of adenosine receptors in high users, resulting in differential contributions of the neural and vascular effects of adenosine in the two study populations.
Yen YF et al. Magn Reson Med. 2002;47(5):921-928
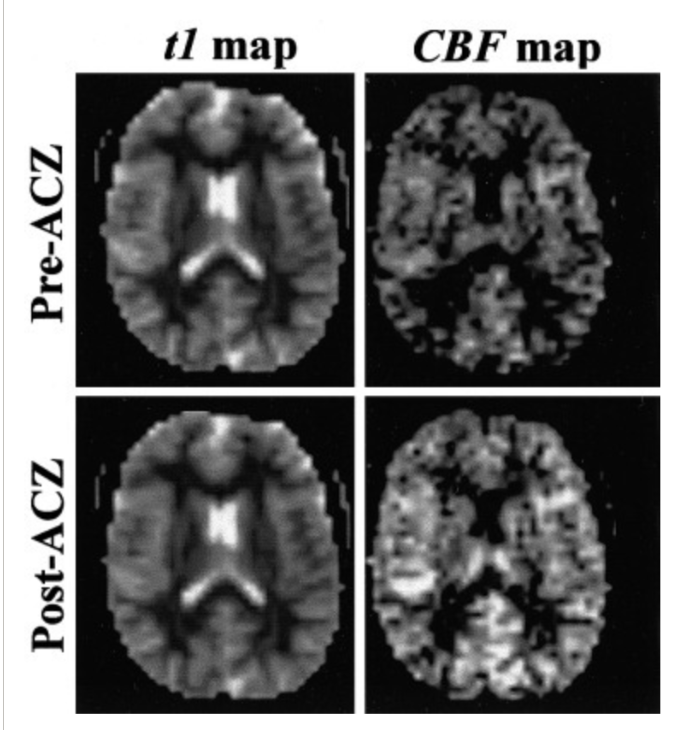
The reproducibility of quantitative cerebral blood flow (CBF) measurements using MRI with arterial spin labeling and acetazolamide challenge was assessed in 12 normal subjects, each undergoing the identical experimental procedure on two separate days. CBF was measured on a 1.5T scanner using a flow-sensitive alternating inversion recovery (FAIR) pulse sequence, performed both at baseline and 12 min after intravenous administration of acetazolamide. T(1) was measured in conjunction with the FAIR scan in order to calculate quantitative CBF. The CBF maps were segmented to separate gray matter (GM) from white matter (WM) for region-of-interest (ROI) analyses. Post- acetazolamide CBF values (ml/100 g/min, mean +/- SD) of 87.5 +/- 12.5 (GM) and 46.1 +/- 10.8 (WM) represented percent increases of 37.7% +/- 24.4% (GM) and 40.1% +/- 24.4% (WM). Day-to-day differences in baseline CBF were -1.7 +/- 6.9 (GM) and -1.4 +/- 4.7 (WM) or, relative to the mean CBF over both days for each subject, -2.5% +/- 11.7% (GM) and -3.8% +/- 13.6% (WM) Day- to-day differences in absolute post-ACZ CBF increase were -2.5 +/- 6.8 (GM) and 2.7 +/- 9.4 (WM) or, relative to the mean CBF increase over both days for each subject, -4.7% +/- 13.3% (GM) and 9.1% +/- 26.2% (WM). Thus, FAIR- based CBF measurements show satisfactory reproducibility from day to day, but with sufficient variation to warrant caution in interpreting longitudinal data. The hemispheric asymmetry of baseline CBF and post-acetazolamide CBF increases varied within a narrower range and should be sensitive to small changes related to disease or treatment.

The corpus callosum is a heterogeneous white-matter tract that connects the cerebral hemispheres. The purpose of this investigation was to study its microstructural architecture in normal human adult brains by using diffusion tensor imaging (DTI). The results of this investigation show a statistically significant increase in anisotropy of the corpus callosum in its more posterior portions compared with its more anterior portions across sex and age groups. Although the microstructural etiology for this apparent increase in anisotropy is unclear, a number of possible mechanisms are presented.
High b-value diffusion-weighted MRI of normal brain
Burdette JH et al. J Comput Assist Tomogr. 2001;25(4):515-519
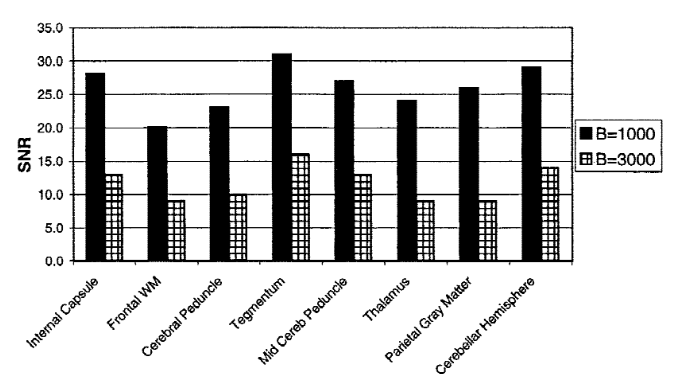
As MR scanner hardware has improved and gradient strengths have increased, we are able to generate higher b values for diffusion-weighted (DW) imaging. Our purpose was to evaluate the appearance of the normal brain on DW MR images as the diffusion gradient strength (“b value”) is increased from 1,000 to 3,000 s/mm2. In order to do this three sets of echo planar images were acquired at 1.5 T in 25 normal subjects using progressively increasing strengths of a diffusion-sensitizing gradient (corresponding to b values of 0, 1,000, and 3,000 s/mm2). All other imaging parameters remained constant, and qualitative assessments of trace images were supplemented by quantitative measures of MR signal and noise in eight different anatomic regions. As a result, gradient strength increased from b = 1,000 to 3,000, both gray and white matter structures diminished in signal as expected based on their relative diffusion coefficients, and the signal-to-noise ratios for the b = 1,000 images were approximately 2.2 times higher than for the b = 3,000 images (p < 0.0001). As the strength of the diffusion-sensitizing gradient increased, white matter became progressively hyperintense to gray matter. Brain DW images obtained at b = 3,000 appeared significantly different from those obtained at b = 1,000, reflecting expected loss of signal from all areas of the brain in proportion to their ADC values. Consequently, when all other imaging parameters are held constant, b = 3,000 DW images appear significantly noisier than b = 1,000 images, and white matter tracts are significantly more hyperintense than gray matter structures.
Diffusion and perfusion MR imaging of cerebral ischemia
Baker MD et al. Ann Thorac Surg. 2000;70(5):1795-1795.
Diffusion and perfusion magnetic resonance (MR) imaging methods have found increasing use for monitoring the effects of cerebral ischemia under clinical and experimental conditions. Blood perfusion can be visualized by either studying the patency of the cerebrovascular bed, recording exchange of diffusible tracers between blood and brain, or measuring the volume and transit time of the circulating blood. Diffusion imaging is based on the modulation of signal intensity by brain water diffusion, and by recording a series of diffusion-weighted images, calculations of the apparent diffusion coefficient (ADC) and the reconstruction of quantitative ADC images can be produced. Brain ADC changes are a sensitive marker of ionic equilibrium, and since disturbances of ion and water homeostasis are among the first pathological alterations induced by brain ischemia, diffusion imaging is able to detect the incipient injury within minutes. Conversely, the reversal of these alterations is able to detect the incipient injury within minutes, and is an early and reliable predictor of postischemic recovery.

Field AS et al. Am J Neuroradiol. 2000;21(8):1388-1396.
Movements of the participant during blood oxygen level-dependent (BOLD) functional MR imaging cerebral activation studies are known to occasionally produce regions of false activation when they are relatively large (>3 mm) and highly correlated with the stimulus. We investigated whether minimal (<1 mm), weakly correlated movements in a controlled functional MR imaging model could produce false activation artifacts that could potentially mimic regions of true activation in size, location, and statistical significance. In order to determine this a life-size brain phantom was constructed. Imaging was performed at 1.5 T using a 2D spiral sequence. Controlled, in-plane, submillimeter movements of the phantom were generated and were made to correlate with a hypothetical “boxcar” stimulus over the range 0.31 < r < 0.96. Regions of false activation were sought using standard statistical methods (SPM96). Results were obtained through a pneumatic system which provided motion control with average in-plane displacements and rotations of 0.74 mm and 0.47 degrees. 18 datasets were analyzed for a statistical threshold of P = .001, with a median number of 3.5 for falsely activated regions, and a mean size of 71.7 voxels. Areas of possibly false activation of average size 72.5 voxels resulting from passive motion of the resting human participant were observed in two of four experiments. Therefore, participant movements of 1 mm or less that are only modestly correlated with a blocked stimulus paradigm can produce appreciable false activation artifacts on BOLD functional MR imaging studies, even when strict image realignment methods are used to prevent them.